Methaemoglobin (MetHb)
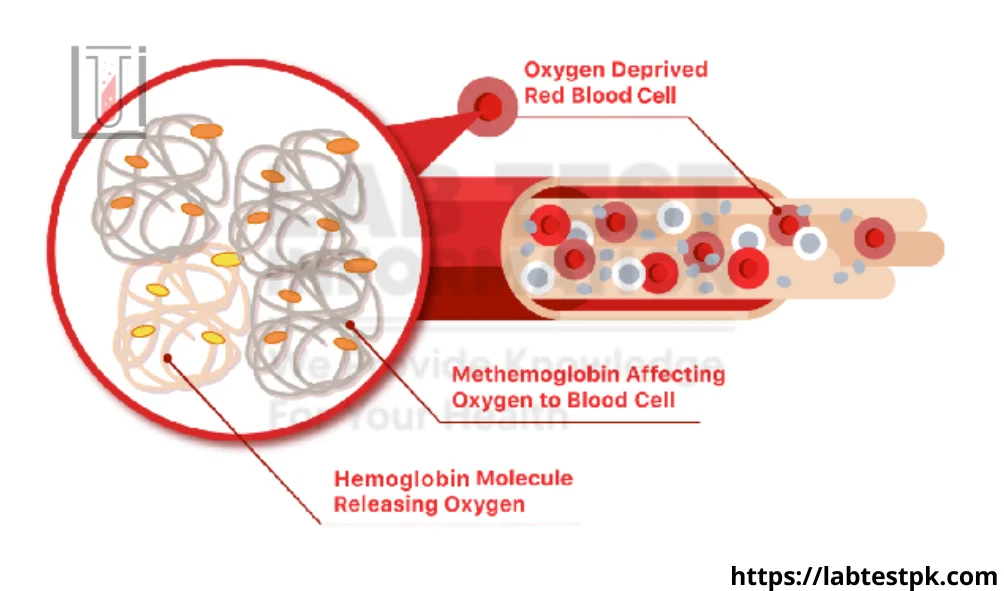
Methaemoglobin (MetHb) is a form of hemoglobin that contains ferric iron (Fe3+) instead of ferrous iron (Fe2+), which is the normal iron form in hemoglobin. Hemoglobin is a protein in red blood cells responsible for carrying oxygen from the lungs to the rest of the body and returning carbon dioxide from the body to the lungs for exhalation.
The iron in hemoglobin normally exists in the ferrous state (Fe2+), which allows it to bind and release oxygen efficiently. However, under certain conditions, the iron can be oxidized to the ferric state (Fe3+), forming methemoglobin. Methemoglobin cannot bind oxygen effectively, and as a result, it reduces the oxygen-carrying capacity of blood.
Some factors that can lead to the formation of methemoglobin include exposure to certain chemicals, drugs, or toxins. For example, certain medications, such as nitrites and certain anesthetics, can induce methemoglobinemia. Additionally, some genetic conditions can predispose individuals to higher levels of methemoglobin.
Causes:
Some of the common causes include:
- Genetic factors: Inherited enzyme deficiencies can result in a higher predisposition to methemoglobinemia. For example, deficiencies in enzymes like NADH-cytochrome b5 reductase can impair the body’s ability to convert methemoglobin to its oxygen-carrying form.
- Medications and chemicals: Certain medications and chemical exposures can induce methemoglobinemia. Some drugs, such as certain anesthetics, antibiotics (like dapsone, and nitrofurantoin), and chemicals (like aniline dyes), can interfere with the normal functioning of enzymes involved in preventing the accumulation of methemoglobin.
- Environmental factors: Exposure to certain environmental toxins and chemicals, such as nitrates and nitrites, can contribute to the development of methemoglobinemia. These substances can be found in contaminated water, certain fertilizers, and certain foods.
- Infections: Some infections, particularly those causing oxidative stress or affecting red blood cell function, can contribute to the development of methemoglobinemia.
- Certain foods: In some cases, consumption of specific foods containing high levels of nitrates or nitrites, such as certain vegetables and cured meats, can lead to methemoglobinemia.
- Foods and drugs during breastfeeding: Infants can be affected if their mothers consume certain medications or foods containing high levels of nitrate or nitrite while breastfeeding.
- She inhaled nitric oxide therapy: In medical settings, the therapeutic use of inhaled nitric oxide can cause elevated methemoglobin levels.
Symptoms of Methaemoglobin (MetHB):
Symptoms of methemoglobinemia can vary depending on the severity of the condition. Mild cases may not cause noticeable symptoms, while more severe cases can lead to significant oxygen deprivation. Some common symptoms include:
- Cyanosis: The most characteristic symptom of methemoglobinemia is a bluish or grayish discoloration of the skin, particularly around the lips and nails, due to the presence of deoxygenated blood.
- Shortness of Breath: As the oxygen-carrying capacity of the blood is compromised, individuals with methemoglobinemia may experience difficulty breathing and shortness of breath.
- Fatigue: Inadequate oxygen delivery to tissues can lead to fatigue and weakness.
- Headache: Insufficient oxygen supply to the brain may result in headaches.
- Confusion or Dizziness: Severe cases of methemoglobinemia can cause neurological symptoms such as confusion or dizziness.
- Increased Heart Rate (Tachycardia): The heart may beat faster in an attempt to compensate for reduced oxygen levels in the blood.
- Seizures: In extreme cases, methemoglobinemia can lead to seizures.
What tests do to diagnose Methaemoglobin (MetHb)?
Here are the key tests used in the diagnosis of methemoglobinemia:
- Co-Oximetry:
- Purpose: Co-oximetry is the most specific test for measuring methemoglobin levels in the blood. It can distinguish between different forms of hemoglobin, including oxyhemoglobin, deoxyhemoglobin, carboxyhemoglobin, and methemoglobin.
- Method: Co-oximetry uses spectrophotometry to analyze the different absorption spectra of hemoglobin forms. It provides a percentage of methemoglobin about the total hemoglobin.
- Arterial Blood Gas (ABG) Analysis:
- Purpose: ABG analysis can provide information about blood gases, including oxygen levels and the oxygen saturation of hemoglobin.
- Method: A blood sample is taken from an artery (usually the radial artery) and analyzed for oxygen and carbon dioxide levels. Methemoglobinemia can result in a decrease in oxygen saturation.
- Standard Pulse Oximetry:
- Purpose: Pulse oximetry is a quick and non-invasive method to estimate oxygen saturation levels in the blood.
- Limitation: Standard pulse oximetry may not accurately reflect methemoglobin levels because it may not differentiate between methemoglobin and other forms of hemoglobin.
- Blood Tests:
- Purpose: Standard laboratory tests, such as a complete blood count (CBC) and blood chemistry, may be conducted to assess overall health and identify potential causes of methemoglobinemia.
- Method: A blood sample is analyzed for various parameters, including the number and types of blood cells, and the levels of electrolytes and other substances.
It’s important to note that co-oximetry is the most reliable method for quantifying methemoglobin levels accurately. Healthcare providers may use a combination of these tests to diagnose methemoglobinemia, assess its severity, and determine the appropriate treatment. Additionally, identifying the underlying cause of methemoglobinemia may involve further investigations, including a thorough medical history and, in some cases, genetic testing.
Treatment:
Here are some general approaches:
- Methylene Blue: Methylene blue is a medication commonly used to treat methemoglobinemia. It acts as a reducing agent, converting methemoglobin back to normal hemoglobin. This treatment is often effective for acquired methemoglobinemia. However, it may not be suitable for certain genetic forms of the condition (like G6PD deficiency).
- Oxygen Therapy: In mild cases, providing high-flow oxygen may be sufficient to alleviate symptoms. This is because oxygen can bind to the remaining normal hemoglobin, compensating for the reduced oxygen-carrying capacity of methemoglobin.
- Ascorbic Acid (Vitamin C): Ascorbic acid can also be used to reduce methemoglobin levels. It is more commonly used in cases where methylene blue is contraindicated or unavailable.
- Exchange Transfusion: In severe cases or when other treatments are not effective, exchange transfusion may be considered. This involves removing the patient’s blood and replacing it with fresh donor blood, effectively diluting the methemoglobin.
- Identifying and Treating Underlying Causes: It’s crucial to identify and address the underlying cause of methemoglobinemia. This could include discontinuing or avoiding medications known to induce methemoglobinemia, treating infections, or managing other contributing factors.
- Avoiding Triggers: For individuals with a genetic predisposition to methemoglobinemia, avoiding known triggers (such as certain medications) is essential.
[…] oxygen from the lungs to the rest of the body and returning carbon dioxide from the body to the lungs for […]
[…] Reaction to Anesthetic: If a local anesthetic is used, there is a very small risk of an allergic reaction, but this is […]
[…] Some women may experience more frequent headaches or migraines when estrogen levels are […]
[…] Flame tests are widely used in chemistry education to demonstrate the concept of atomic emission spectra. They provide a visual and engaging way to teach students about the behavior of electrons and the […]
[…] underlying conditions. It’s often the body’s way of getting rid of harmful substances, toxins, or irritants from the […]
[…] elastase. When there is a deficiency of alpha-1 antitrypsin, the elastase can cause damage to the lung tissue, leading to conditions such as chronic obstructive pulmonary disease (COPD), emphysema, and chronic […]
[…] Holter monitoring […]